Introduction
Patients now interact with conversational AI before they ever speak to a person. They book appointments at midnight, describe symptoms through a chat window, get medication reminders after discharge, and resolve billing questions without sitting on hold.
For clinicians, the same technology surfaces drug interaction data mid-consultation and handles documentation that used to consume hours of their day.
The scale of this shift is real. According to Grand View Research, the global conversational AI in healthcare market stood at $13.68 billion in 2024 and is projected to reach $106.67 billion by 2033 — driven by genuine clinical adoption across scheduling, triage, documentation, and patient engagement.
Yet most healthcare founders, operators, and product teams deploying these systems don't fully understand what's actually running underneath. That gap produces poor vendor decisions, compliance exposures, and systems that frustrate the patients they were built to help.
This guide covers how conversational AI in healthcare actually works: the mechanics, the use cases, the compliance requirements, and what it takes to build something that holds up in production.
Key Takeaways
- Conversational AI uses NLP, machine learning, and LLMs to handle natural, medically relevant dialogue across patient and clinical touchpoints
- The system runs a multi-stage pipeline: language understanding → intent recognition → backend integration → response generation
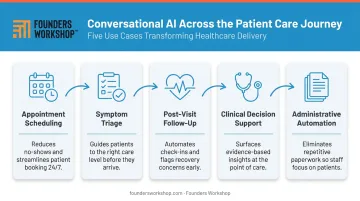
- Core use cases include scheduling, symptom triage, post-visit follow-up, clinical decision support, and administrative automation
- HIPAA-compliant architecture, EHR integration, and audit-ready logic are non-negotiable for production healthcare deployments
- Healthcare deployments are custom engineering projects where compliance and data handling architecture must be defined at the start, not retrofitted
What Is Conversational AI in Healthcare?
Conversational AI is software that enables machines to understand and respond to human language. In healthcare, that means systems capable of handling clinical and administrative communication — through text or voice — with patients, providers, and staff.
It exists because the operational gaps are real. The AHA's 2025 Workforce Scan reports that 88% of nurses worry staffing shortages affect patient care, and HRSA data shows roughly 75 million people live in primary care shortage areas. Front desks are overwhelmed. Patients need access after hours. Repetitive administrative queries consume staff bandwidth that should go elsewhere.
What It Is Not
Three categories are frequently conflated — and the distinction matters for deployment:
- Rule-based chatbots — scripted decision trees with fixed paths; predictable but rigid
- Diagnostic AI tools — imaging analysis, clinical decision engines; not the same as conversational systems
- Conversational AI — NLP-driven, context-aware, capable of handling variable inputs
Mixing them up leads to wrong deployment expectations and underbuilt systems.
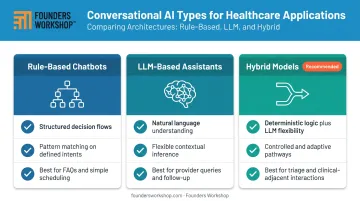
Three Types Used in Healthcare Today
| Type | How It Works | Best Suited For |
|---|---|---|
| Rule-based chatbots | Structured flows, pattern matching | FAQs, simple scheduling, intake forms |
| LLM-based assistants | Natural language, flexible inference | Provider queries, follow-up conversations |
| Hybrid models | Deterministic logic + LLM flexibility | Triage flows, clinical-adjacent interactions |
Hybrid models have become the practical standard for safety-sensitive healthcare contexts: they preserve the LLM's flexibility for natural conversation while using deterministic logic where clinical accuracy is required.
How Conversational AI Works in Healthcare
Conversational AI in healthcare isn't a single model sitting in a box. It's a coordinated pipeline of stages, each responsible for a specific layer of processing, logic, and output.
Input Processing and Language Understanding
The system receives raw input — typed text, a voice message, or structured form data — and converts it into something a machine can work with. For voice, Automatic Speech Recognition (ASR) handles the transcription. For text, Natural Language Processing (NLP) breaks the input down into tokens, entities, and linguistic intent.
Healthcare language is harder than general conversation. It includes drug names (brand and generic), clinical abbreviations, misspelled symptom descriptions, and emotional context that shifts meaning.
General-purpose NLP models underperform in clinical settings for exactly this reason. Models fine-tuned on healthcare-specific data — like BioBERT or ClinicalBERT — handle these inputs with measurably better accuracy.
Intent Recognition and Context Management
Once the input is understood, the system identifies what the user actually wants: schedule an appointment, ask about a medication, report a worsening symptom. That intent maps to a predefined or learned action.
Context windows allow the system to track prior conversation turns — so when a patient says "Can I change that?" the system knows what "that" refers to.
This is where rule-based and LLM-based systems diverge sharply:
- Rule-based: matches patterns to intents; reliable, but breaks outside defined paths
- LLM-based: infers meaning from context; flexible, but less predictable
For healthcare, that tradeoff matters. Reliability often wins in clinical workflows.
Backend Integration and Action Execution
Understanding intent has no value unless the system can act on it. This layer connects to external platforms:
- EHR systems (reading patient records, writing back updates)
- Scheduling tools (checking availability, confirming bookings)
- Billing and insurance systems
- Live agent routing when escalation is needed
This integration layer is one of the most technically complex parts of any healthcare deployment. It requires secure API connections, role-based access controls, and data handling that complies with HIPAA. CMS interoperability rules now mandate HL7 FHIR APIs for impacted payers, making FHIR-compliant endpoints the standard path for structured healthcare data exchange.
Response Generation and Delivery
The system formulates its reply. For rule-based systems, this is a retrieved or templated response. For LLM-based systems, it's a generated response — ideally grounded in retrieved clinical or operational data to reduce the risk of hallucinations.
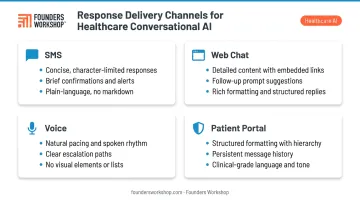
Responses are delivered across channels, and each one behaves differently:
- SMS: must be concise — a three-paragraph symptom response does more harm than good
- Web chat: can carry more detail, links, and follow-up prompts
- Voice: requires natural pacing and clear escalation paths
- Patient portals: benefit from structured formatting and persistent message history
Channel-specific behavior matters more than most teams expect. Matching response format to delivery channel is as important as getting the content right.
Key Use Cases of Conversational AI in Healthcare
Conversational AI creates value at specific, high-friction points in the care journey. The most productive implementations target one or two of these areas first rather than trying to automate everything simultaneously.
Appointment Scheduling and Patient Access
Conversational AI can handle the entire scheduling loop: intake, availability checking, confirmation, rescheduling, and reminders — without staff involvement. This matters because 71% of practices had fewer than 25% of patients using digital self-scheduling tools as of 2025, meaning significant demand exists that current tools aren't capturing.
Automating this channel reduces front-desk call volume and extends access to patients who can only engage outside business hours.
Symptom Triage and Care Routing
AI-guided triage walks patients through structured symptom assessments and recommends the appropriate level of care — self-care, virtual visit, urgent care, or ER. The logic here must be deterministic and auditable. Research comparing general LLMs to supervised triage tools shows a clear gap: unsupervised general models should not be used as standalone triage engines. The triage flow needs constrained, validated decision paths, not freeform generation.
Post-Visit Follow-Up and Chronic Care Management
This is where conversational AI can have meaningful clinical impact. Medication nonadherence costs the US healthcare system an estimated $100 billion to $300 billion annually according to the CDC. Automated follow-up conversations, covering recovery check-ins, medication adherence prompts, and escalation triggers when responses indicate concern, extend the care relationship beyond the visit without adding staff burden.
Clinical Decision Support and Administrative Automation
On the provider side, conversational AI lets clinicians query drug interaction data, clinical guidelines, and relevant literature through natural language rather than manual documentation searches. As LLMs improve on clinical benchmarks, this use case is gaining traction — though human oversight remains non-negotiable.
Administrative workflows are equally well-suited for automation. Common targets include:
- Billing inquiries and insurance verification
- Patient intake collection
- Record updates and documentation
Automating these tasks reclaims staff time and reduces the friction patients encounter at non-clinical touchpoints.
Compliance, Security, and Risks in Healthcare Conversational AI
Inaccurate outputs or insecure data handling in healthcare don't just create bad user experiences. They can cause patient harm or trigger regulatory liability.
HIPAA Compliance and Data Architecture
HIPAA compliance for a conversational AI system means specific, technical requirements — not a checkbox on a vendor form:
- Encryption: PHI must be protected in transit and at rest
- Access controls: Only authorized users and service accounts can reach patient data
- Audit logging: Every interaction touching PHI must be logged and reviewable
- Business Associate Agreements: Every vendor processing PHI — including LLM providers, hosting platforms, analytics tools — requires a BAA
HHS updated its guidance in 2024 to clarify that tracking technologies on symptom or chat pages may expose organizations to HIPAA liability if those tools transmit PHI to third parties. Session replay tools and unreviewed analytics scripts on patient-facing pages are a real risk area many teams miss.
Auditability, Hallucination, and Clinical Risk
Healthcare organizations need to trace every decision their AI system makes. That requires full conversation logging, decision path visibility, and the ability to reproduce how a specific response was generated.
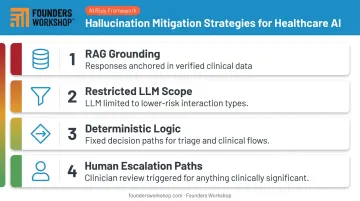
Auditability concerns connect directly to hallucination risk. An npj Digital Medicine study reported 1.47% hallucination and 3.45% omission rates in medical text summarization — numbers that sound small until you consider the interaction volume inside a health system. Mitigation strategies include:
- Grounding responses in retrieved, verified clinical data (RAG)
- Restricting LLM use to lower-risk interaction types
- Using deterministic logic for triage and clinical flows
- Building human escalation paths for anything clinically significant
Health Equity and Regulatory Landscape
Conversational AI can widen healthcare disparities if not designed for diverse populations. Adults with limited English proficiency face documented barriers to digital health tools, and populations with low digital literacy or older patients may disengage from poorly designed interfaces. Multilingual support, simple language settings, voice options, and accessibility testing are functional requirements, not optional enhancements.
The regulatory landscape is also moving fast. Key developments to track:
- FDA final guidance (December 2024): Predetermined Change Control Plans now apply to AI-enabled device software
- ONC HTI-1 rule: Establishes transparency requirements for AI in certified health IT
Organizations building patient-facing clinical functions should monitor both — and build governance processes (bias audits, clinical validation) into the product lifecycle from day one.
Building Conversational AI for Healthcare: What It Actually Takes
Building a production-grade conversational AI for healthcare is a custom engineering project. The combination of compliance requirements, EHR integration complexity, and the need for auditable logic means off-the-shelf tools rarely cover the full picture without significant configuration or custom development work.
The decisions that matter most happen early:
- Define scope first — choose one or two use cases to automate; scheduling and follow-up reminders are lower-risk starting points than triage
- Choose your architecture — rule-based, LLM-based, or hybrid; the choice should reflect the clinical risk level of each interaction type
- Map your integrations — identify which EHR and backend systems need to connect, and assess FHIR endpoint availability early
- Enforce compliance at the infrastructure level — encryption, access controls, audit logging, and BAAs need to be in the architecture from day one, not added later
Healthcare organizations and health-tech startups frequently underestimate how much the compliance and integration layers add to scope. A focused MVP covering scheduling and reminders with proper compliance infrastructure is a different build than what most teams initially sketch out.
That scope gap is where many projects stall. Working with a development partner that has built HIPAA-compliant healthcare applications before — EMR integrations, telemedicine platforms, patient communication tools — shortens the path considerably.
Founders Workshop has delivered that kind of work since 2008. Their structured 5D Process takes projects from validated concept through deployment, with compliance architecture built in from the start rather than retrofitted after the fact.
Frequently Asked Questions
What is the difference between a healthcare chatbot and conversational AI?
Rule-based chatbots follow scripted decision trees — they only handle inputs they were explicitly programmed for. Conversational AI is dynamic, NLP-driven, and context-aware. All chatbots are a subset of conversational AI, but not all conversational AI is a simple chatbot.
Is conversational AI in healthcare HIPAA compliant?
HIPAA compliance depends entirely on how the system is designed and deployed. It requires encrypted data handling, role-based access controls, audit logging, and signed Business Associate Agreements with any vendor processing PHI. "HIPAA compliant" is an architectural outcome, not a vendor claim.
How does conversational AI integrate with EHR systems?
Integration happens via secure APIs — typically FHIR-compliant endpoints — that allow the AI system to read patient data, write updates, and trigger workflows within the EHR. This integration layer is technically complex and vendor API coverage varies significantly, so scoping it early is critical.
Can conversational AI replace doctors or clinical staff?
No. It handles repetitive, high-volume communication tasks — scheduling, reminders, administrative queries — not clinical judgment. Best-practice implementations keep licensed staff in the loop for any interaction that could affect patient safety.
What are the biggest risks of using conversational AI in healthcare?
The primary risk areas to plan for:
- AI hallucination — inaccurate medical information generated with false confidence
- Unsecured PHI — improper data handling that creates HIPAA exposure
- Health equity gaps — systems that exclude non-English speakers, elderly users, or patients with limited digital literacy
How long does it take to build a conversational AI solution for healthcare?
A focused MVP covering one or two use cases with proper compliance infrastructure typically takes 3–6 months. More complex systems with deep EHR integration and triage logic take longer — scope, PHI handling requirements, and integration depth are the primary timeline drivers.